
Note: This article is the opinion of an expert. Please note that this is not the opinion of the COVID-19 Advisory Panel.
This article is a personal written opinion submitted to the Cabinet Secretariat on May 25, 2022, prior to the compilation of the report of the “Expert Meeting on Novel Coronavirus Disease Control” (Chairman Ryozo Nagai) held at the Cabinet Secretariat from May to June 2022. This article compiles the issues related to the Infectious Diseases Control Law, Special Measures Act, and its operations; infrastructure, gathering, and publication of information; as well as the ideal state of Public Health Centers, research, expert advisory organizations, contingency legislation, and the command center. In addition, the Chairman explained about this written opinion, of which copies were given to the reporters, at a press conference on June 21 for about an hour.
Executive Summary
The number of COVID-19 cases and fatalities in Japan are lower than that in major countries, and the measures implemented appear to be successful. However, this is largely due to the efforts provided at the point of care and the high level of public health awareness of the public. At the same time, the medical care provision system was under extreme pressure; a huge burden was placed on infection prevention sites and medical care site, and restrictions on the lives of the public continued. Some have also pointed out the low numbers of PCR testing, the actual situation of the community-acquired infections was not fully understood, and that prompt decision-making was difficult with the request-based measures (Japan model). To boost public acceptance, there is a need to review the measures taken by the Japanese government thus far and prepare for the next major pandemic based on the lessons learned.
1) Issues with the legal system for public health contingencies and its operation
- COVID-19 disease control and prevention measures have revealed many issues with the infection prevention activities at Public Health Centers and the securing of necessary hospital beds. Although these are enforced under administrative authority based on the “Act on the Prevention of Infectious Diseases and Medical Care for Patients with Infectious Diseases” (“Infectious Diseases Control Law”), the functions and capacity of the public health system, mainly Public Health Centers, mentioned in the Infectious Diseases Control Law are limited, and often led to confusion in the Public Health Centers and at the point of care. In addition, although the “Act on Special Measures for Pandemic Influenza and New Infectious Diseases Preparedness and Response” (“Special Measures Act”) stipulates that the prefectural governors may issue orders to physicians and healthcare professionals, a lot of coordination is required to secure hospital beds through administrative authority, including the dispatch of physicians and nurses and the transfer of inpatients. There is therefore a need to establish a corresponding structure and rules from normal times.
- Since the number of cases will fluctuate depending on the mutation of the viral genome and the peaks of the seasonal outbreaks, it is essential to take prompt actions depending on the situation regardless of how the cases are classified under the Infectious Diseases Control Law. Indicators and guidelines should be developed for this purpose as well. Further, infection rate and severity of COVID-19 disease, and the impact of the infection control measures on daily life vary greatly from generation to generation. It is critical to listen to the opinions of various generations when taking measures.
2) Issues with the medical care provision system and functions of Public Health Centers
- The number of inpatient beds in Japan is one of the highest in the world. However, 80% of the hospitals are private. Moreover, the number of physicians and nurses per bed is as low as half to a fifth of the number in Europe and the United States because medical resources such as hospital beds and personnel are spread widely and thinly. While this is a convenient system from normal times due to its guaranteed free access to medical care, it is difficult to care for critically ill patients during a pandemic outbreak, and medical resources have to be reallocated to appropriately respond to the pandemic. However, hospitalization measures under the Infectious Diseases Control Law mean that “medical care by administrative authority” may supersede the “medical care based on the consent of the medical institution and the patient”, of which the latter has been generally practiced in Japan. The sharing of information and fine-tuning of the delivery of point of care are therefore indispensable.
- In recent years, there has been a significant decline in the number of Public Health Centers, which are at the forefront of infection prevention. On the other hand, the increase in day-to-day operations and delays in the adoption of IT left the centers with little resources to spare on preventing infections. The advent of the pandemic in this state thus placed a heavy burden on the point of care. In particular, depending on the type of Public Health Centers established, they sometimes fall into the administrative gap between that of prefectural and municipal governments. Some Public Health Centers therefore had to be responsible for tasks that were not part of their original operations, such as securing food for those waiting at home for hospitalization. Legislation for contingencies is therefore necessary to ensure that the division of operations and coordination can proceed smoothly.
3) Issues with the testing system
- Testing is the cornerstone to protecting against infection and diagnosis. Japan was late to establish a PCR testing system as the SARS and MERS pandemics did not happen in Japan. This was why testing was prioritized for populations that were highly likely to be positive. Meanwhile, the number of cases was only determined by administrative testing, and neither sentinel surveillance nor active surveillance was conducted. In addition, private testing and free PCR testing that were conducted in various regions are considered beyond the jurisdiction of administrative testing, and the positivity rate of these tests are rarely disclosed. There was also no tracing of those who tested positive. And during that time, the sixth wave saw an explosive increase in the number of infections, especially amongst young children and schoolchildren.
- In order to use PCR testing to prevent the spread of infectious diseases, we must first ensure that there is enough capacity for testing. On top of that, it is essential to carefully consider the false positive rate when developing a testing strategy. The testing policies also need to be reviewed according to the spread of the infectious diseases and the testing capacity, and experts are expected to provide appropriate explanations and advice.
4) Issues in gathering and publication of information
- Experts have to work with many researchers in order to understand the situation of infection and pathophysiology, to analyze viral mutations, and treatment effects. However, the epidemiological information, samples, and genomic information provided by the point of care to expert advisory board during a pandemic was not always sufficient. For instance, even though the data and samples were collected by the National Institute of Infectious Diseases, it was sometimes not possible to provide information or specimens to third parties. This may be due to the provider’s preference to protect the personal information. In a state of emergency, the point of care should have a system to facilitate the provision of data and samples without being overly mindful of the Act on the Protection of Personal Information.
- There are also many problems with the publication of information. The national government, prefectures, and research institutions did not employ a standardized method for data disclosure, which made it difficult to conduct time series analysis of data. The methods for data disclosure should be reviewed and instead of cross-sectional data, primary data files should be provided to allow researchers to conduct time series analysis of data from multiple angles.
- During a pandemic, the construction of a data lake that allows for agile and flexible analysis is especially important. And it is no mean feat. Assuming that the data will be used by researchers in diverse specialties, database specialists and healthcare professionals need to work together to come up with a data structure that enables the combination and analysis of diverse data, as well as consider the design for this purpose from normal times. This is also crucial for data sharing and risk communication.
- Problems also continue to appear in the infection control applications such as HER-SYS, a health center real-time information-sharing system on COVID-19 infected cases, and COCOA, a COVID-19 contract tracing application. Japan is severely behind other countries in the reform of information systems; medical institutions and Public Health Centers still have to rely on fax machines in order to communicate with each other. There is an urgent need to reform the medical care information system to prepare for the next pandemic.
- There are many issues with the transmission of information as well. It is necessary to “publish easy-to-understand information” not only for the public, but also for foreign nationals in Japan and abroad.
5) Ideal state of expert advisory board
- During the COVID-19 outbreak, even experts may not necessarily be able to rely on their previous experience and knowledge; there is a need to respond according to the situation. For instance, the ideal way to conduct PCR testing and active epidemiological investigations should differ depending on whether it’s during the early outbreak phase or the epidemic phase. It is hard to say that the switch in policy was made in a timely manner. There were also opinions that the models used to predict the outbreaks were unsatisfactory. It is therefore important for expert advisory board to nominate flexible thinkers from diverse backgrounds with a wealth of research experience, and to create an atmosphere where people can discuss without any inhibitions or restrictions. Expert advisory board should also guide domestic epidemiological and clinical research as well as create a system for local researchers to collaborate with external scientific groups through data centers.
6) Issues with infectious diseases research system
- During the COVID-19 outbreak, the number of papers from Japan was among the lowest among developed countries. This was not only because researchers did not have access to information and samples, but also because a system for conducting epidemiological and clinical research was simply not in place. The quality of scientific advice will deteriorate if progresses are not made in domestic investigations and research. In addition, vaccines and therapeutic drugs could be rapidly developed in other countries due to their strong foundation of basic research in infectious diseases and human resource development. In Japan, the budget for basic research on infectious diseases is small, and human resource development is inadequate. There is a need to strengthen basic research, including international joint research, in the future.
7) Ideal state of command center
- Various zoonotic diseases, including coronaviruses, are foreseen to continually lead to pandemics in future. There is a pressing need to develop legislations, create systems, and boost research capabilities for public health contingencies. The fundamentals of pandemic measures are to gather the necessary information from the necessary locations using multiple methods and distribute the burden. Also, the measures should be a combination of multiple methods instead of a single one. The fact that Japan has not properly implemented these measures means that the functions of the command center must be strengthened from now on. There is a need to, however, have a deep debate concerning the establishment of laws and governance, and the ideal state of governance institutions. For the sake of discussion, it is desirable to thoroughly review how the information should be gathered during the pandemic, ideal state of data centers, data utilization, and the ideal way to go about publishing information during the pandemic.
This pandemic is a completely new experience for everyone and errors in judgment are inevitable. It is important not to point fingers at each other for the errors, but to respond to the situation in a flexible manner, do all in our power at that time, and explain the situation and policies to the public in an easy-to-understand manner.
The debate over COVID-19 measures is not limited to the issues surfaced in the infection control measures and crisis management in Japan. It is also a question of how to control and come to terms with complex phenomena that cannot be handled by rationalism alone. It includes information infrastructure, data-driven thinking, analysis and predictions, information sharing, information publication, accountability, social disparities, reputational damage, mutual aid and mutual assistance, as well as scientific advice and the ideal state of scientific research, and wisdom, technology, and other issues that should be resolved to survive in uncertain times. We hope that these will be continuously and multilaterally examined from various perspectives and situations in the future.
Introduction
The number of COVID-19 cases and fatalities in Japan far less than in Europe and the United States. This is thought to be due to those involved in providing medical care and engaged in measures to prevent the spread of infection, as well as the high level of public health awareness of the public, and our deepest respect goes to all those who were involved. However, the repeated mutations in SARS-CoV-2 virus have expanded the scale of the outbreak. The recurring pandemic waves have significantly impacted not only the prevention of infection and point of care, but also the medical care provision system and the socioeconomic activities of the people. To boost public acceptance, it is essential to review the COVID-19 measures taken by the Japanese government thus far and prepare for the next pandemic based on the lessons learned.
The COVID-19 pandemic has pushed everyone into an unknown territory, and the experience and knowledge accumulated thus far have not always been useful. In order to make appropriate decisions and take preventive measures in such situations, we need to be prepared for states of emergency from normal times. A report examining Japan’s response to pandemic after the outbreak of the novel influenza (A/H1N1) in 2009 was compiled (1). Yet the recommendations made in the report were not fully utilized when preparing for this pandemic. The government’s explanation of COVID-19 measures has exposed issues in the country’s infection control measures and crisis management systems that may require more in-depth scientific discussion.
Various opinions on the governments’ responses to the COVID-19 pandemic have already been expressed in Europe and the United States (2-6). In particular, the United Kingdom parliament took the lead in conducting an inquiry into their response and published the report in November 2021 (6). While an independent investigation commission in Japan has published a report on their inquiry into the country’s handling of the pandemic in August 2020 after the first wave ended (7), no new inquiries have been conducted since then. This “Expert Meeting on Novel Coronavirus Disease Control” was organized to gather opinions on the responses taken to date based on the “Act on Special Measures for Pandemic Influenza and New Infectious Diseases Preparedness and Response” (“Special Measures Act”), the establishment of a healthcare delivery system, as well as issues related to these responses from a medium- to long-term perspective. The first meeting was held on May 11, 2022, and after two rounds of interviews, the report will be compiled in June. It is necessary to continue conducting inquiries into the policies across a wide range of areas. But as the pandemic continues, it is somewhat meaningful and important to hear the opinions of all levels of society at this time, even if it is a government-led inquiry. However, due to the short inquiry period, each member was asked to first submit their written opinions that would be subsequently reflected in the compiled report.
In this written opinion, I will give my opinions as well as personal analysis about the 1) Issues with the laws regarding COVID-19 pandemic measures and administrative response, 2) ideal state of expert advisory board, 3) issues with research systems, 4) issues with the infrastructure and presentation of information, and 5) ideal state of command center.
1 Issues with the laws regarding COVID-19 pandemic measures and administrative response
The COVID-19 measures are primary enforced under administrative authority based on the “Act on the Prevention of Infectious Diseases and Medical Care for Patients with Infectious Diseases” (“Infectious Diseases Control Law”) and Special Measures Act. Under the Infectious Diseases Control Law, the authority is concentrated in the prefectural governors who have jurisdiction over the Public Health Centers and are able to impose restrictions on work attendance and other measures. Meanwhile, physicians and administrators of medical institutions are responsible for cooperating with the necessary measures taken by the government and local public bodies to prevent the outbreak and spread of infectious diseases. COVID-19 is positioned as a novel influenza infection, and the details of infection prevention measures are stipulated in the Law (Figure 1). Under this system, “medical care by administrative authority” may supersede the “medical care based on the consent of the medical institution and the patient”, of which the latter has been generally practiced in Japan. Significant fine-tuning of the delivery of point of care, including preliminary meetings, are therefore indispensable.
 |
| Figure 1: Positioning of COVID-19 in the Infectious Diseases Control Law and details of the measures Source: Ministry of Health, Labour and Welfare materials (2021.12.17) https://www.mhlw.go.jp/content/10906000/000868295.pdf |
1) Issues with the administrative authority
Under the Infectious Diseases Control Law, physicians must file notifications about COVID-19 cases with the Public Health Centers. COVID-19 cases are also subjected to active epidemiological investigation, restrictions on work attendance, hospitalization measures, specimen collection, and they are to follow the orders of the Public Health Centers. For hospitalization measures, despite the fact that the cooperation was requested to secure hospital beds under Article 16(2) of Infectious Diseases Control Law, the number of infected cases who were forced to stay at home because they could not find a place to be hospitalized increased when the pandemic was spreading. In contrast to this, Article 31(1) of Special Measures Act stipulates that “when the need to provide medical care to patients is recognized, prefectural governors may request or order physicians, nurses, or other healthcare professionals to do so for said patients, etc., indicating the place, period, and other necessary matters”. Despite that, this provision was not utilized. Even if hospital beds are secured through administrative authority, a lot of coordination, such as the dispatch of physicians and nurses and the transfer of inpatients, is required. Above all, despite the fact that Japan has one of the highest numbers of inpatient beds in the world, 80% of the hospitals are private. The number of physicians and nurses per bed is also as low as half to a fifth of the number in Europe and the United States because medical resources such as hospital beds and personnel are spread widely and thinly. While this system is convenient from normal times due to its guaranteed free access to medical care, it is difficult to care for critically ill patients during a pandemic outbreak, and medical resources have to be reallocated to appropriately respond to the pandemic. There is therefore a need to establish a corresponding structure and rules from normal times.
Actual infection control measures should be based on the measures in Figure 1, but also be flexible according to the situation of the outbreaks, local conditions, and response capabilities. For instance, under the current Infectious Diseases Control Law, Public Health Centers are responsible for issuing recommendations for hospitalization and taking measures when COVID-19 cases are diagnosed. Yet the functions and capacities of the public health system delivered mainly through the Public Health Centers were limited, and confusion often arose at the point of care.
Since the hospitalization measures taken by the administrative organs should be intended to prevent the spread of infection, everyone who tested positive for infections should be hospitalized and quarantined. But because an extremely high number of people tested positive, the infected cases were instead assigned to their residences, in-residence care facilities, or hospitalized in medical institutions based on their symptoms and risks of developing severe complications. In some cases, it was difficult to coordinate hospitalization, and this led to the public’s criticism of the segregation between public health and medical care. On the other hand, some mild COVID-19 cases were forced to be hospitalized in medical institutions for reasons such as “at risk of developing severe complications”. This is overtriage, and will in turn reduce the number of hospital beds that can be secured. Instead of a rigid response based on the type of disease according to the Infectious Diseases Control Law, Public Health Centers and medical institutions should create a system allowing for flexible and collaborative responses according to the situation, to which the corresponding indicators should be developed.
The nature of the outbreak fluctuates greatly depending on the emergence of variants and the vaccination situation. Looking at the infection rates by age group in particular revealed that up to the fifth wave, those in their 20s had the highest infection rates, followed by those in their 30s and teens (Figure 2). But the sixth wave saw a sharp increase in the infection rate among minors, with 10.4% of those under the age of 10 being infected between January and May of this year (Figure 3).
 |
| Figure 2: Number of new cases per 100,000 people by age group (prepared by Visiting Professor Senichi Obayashi, Jichi Medical University). The left graph shows the number of new cases in their 40s and younger, and the right graph shows the number of new cases in their 50s and older. The infection rate is high among those in their 20s in the fifth wave and those under the age of 10 in the sixth wave. Calculated using newly confirmed cases (https://covid19.mhlw.go.jp/) aggregated by week, age group and sex released by the Ministry of Health, Labour and Welfare, as well as population statistics by age group from 2020 Population Census published by the Statistics Bureau, Ministry of Internal Affairs and Communications (https://www.stat.go.jp/data/jinsui/index2.html#suikei). |
 |
| Figure 3: Infection rates by age group for each wave of the outbreak (prepared by Visiting Professor Senichi Obayashi, Jichi Medical University). The left graph shows the infection rates by age group during the third wave (blue), fourth wave (orange), and fifth wave (gray), while the right graph shows the infection rates by age group during the sixth wave. The number of cases increased dramatically in the sixth wave, with 10.4% of those under the age of 10 being infected. |
If the pandemic is approaching community transmission levels, and the inter-generational transmission, mode of transmission, and hot spots undergo dramatic changes, sentinel as well as active surveillance are also required within the framework of active epidemiological investigation as stipulated in the Infectious Diseases Act. A system should be established to perform PCR testing even in asymptomatic cases as well as subgroup analyses of positivity rates and Ct values (the number of amplification cycles required to create enough copies of the viral DNA to be detected; the lower the Ct value, the higher the viral load) by parameters such as age group, work place, region, and school. But sentinel surveillance has not been performed since all new COVID-19 cases were reported, and even active surveillance is not performed because it is not stipulated under the current Infectious Diseases Control Law. A government expert panel proposed the need for surveillance in May 2020, to which it has been implemented in Mie Prefecture (8, 9).
2) Issues with information gathering
There are also many issues with how the information was gathered by the government. Article 6(2) of Special Measures Act stipulates that the “gathering of information on the status of outbreaks, progress, and causes of novel influenza, etc. in other countries and Japan” as one of the matters prescribed in the National Action Plan, while Chapter III of Infectious Diseases Control Law has a series of provisions on the gathering and publication of information on infectious diseases. Nevertheless, the local governments have stated that the Act on the Protection of Personal Information has made it difficult for them to provide epidemiological data gathered at the point of care and specimens collected from infected cases to government expert meetings and researchers. On top of that, even if the Public Health Centers and Public Health Institutes provided the information and materials to the National Institute of Infectious Diseases, the data could not be published or provided to third parties without the consent of local governments. There have been cases where even panel members were unable to access the original data for expert meetings and had to provide their analyses based on press information. There is a need to revise the Act so that local governments can promptly provide information with a peace of mind without fear of violating the Act on the Protection of Personal Information (Prefectural Ordinance). A case in point on this subject is the revision of the Basic Act on Disaster Management based on the lessons learned from the Great East Japan earthquake. This Act stipulates that municipalities may provide Lists of Residents in Need of Assistance in Evacuation to external parties without the consent of the individual if it is deemed necessary to protect the lives and bodies from disaster, providing legal standing for the provision of personal information during emergencies.
During a pandemic, it is crucial to set up a data center that gathers and analyzes data; the system and format for the data center have to be prepared in advance from normal times.
3) Issues with the system of the Public Health Centers
Under the current Infectious Diseases Control Law, Public Health Centers are at the forefront of infection prevention measures. Yet the number of Public Health Centers (about 850 of them in 1996) has been rapidly declining since 1997; as of 2022, there are only 468 Public Health Centers left. While the number of centers was decreasing, there were delays in the adoption of IT and the regular operations was increasing. Burdened with excessive duties without a contingency system, the Public Health Centers struggled to cope with the pandemic (10).
Public Health Centers are responsible for preventing the spread of infection. Yet the command center responsible for preventing this did not issue clear directives, and the chain of command from the national government, prefectural governors, special wards, and mayors of the cities in which the Public Health Centers were established, was not functioning properly. This forced the Public Health Centers to coordinate their operations across the jurisdiction of different ministries and agencies. The combination of these factors put a strain on the operations of the Public Health Centers. During the waves of the outbreak, Public Health Centers had to handle complaints, perform triage, arrange for patient transport, and even arrange meals for those waiting at home for hospitalization. The medical professionals also could not carve out time to devote to public health measures (10).
The Action Plan of municipalities based on the Special Measures Act did not work out. The Public Health Centers established in the prefectures thus fell into the administrative gap between the prefecture and the city, and had to shoulder a huge amount of workload related to infection control and hospitalization measures. Even though the mayor of the municipality is responsible for the protection of the lives of the residents, a problem lies in the fact that the role of the municipality is not specified in the Infectious Diseases Control Law.
Other issues include the revision of the roles and functions of Public Health Centers from normal times and emergencies based on the relevant acts and regulations, IT reform in Public Health Centers, and the creation of a system that will enable other departments and contractors to carry out the operations of Public Health Centers. There is a need to promote a flexible employment system in Public Health Centers and develop human resources of public health physicians. It is also imperative to clarify the position of Public Health Centers stipulated in the Community Health Act; the position of Public Health Institutes, whose establishment is left to local governments; and the position of municipalities with regard to infection control measures (11). It is also important for the Ministry of Health, Labor and Welfare and the Fire and Disaster Management Agency to discuss the transfer as well as point out the principles of transferring infected patients from normal times.
At present, the Public Health Centers are currently Japan’s system of promoting health and handling infectious diseases during normal times, and it is clear that they are unable to cope with the rapid and large-scale spread of infection like the fifth and sixth waves. There is an urgent need to create a system that is equipped to respond to disasters.
4) Issues with PCR testing
Article 8(3) of Infectious Diseases Control Law stipulates that “the asymptomatic carriers of a novel influenza infection, etc. are deemed as patients of the novel influenza infection, etc. respectively, and the provisions of this Act apply”. In reality, the clinical sites see many cases with unknown infection route (9), and often witness household transmission from asymptomatic positive cases. PCR testing should therefore be performed to identify asymptomatic carriers as well as symptomatic cases. As a matter of fact, Japan was late to establish a PCR testing system as the SARS and MERS pandemics did not happen. Especially when the pandemic first broke out in the first half of 2020, PCR test kits and testing systems were not available, and testing was only conducted on a limited number of people. This was why testing was prioritized for infected cases and their close contacts. Although private testing developed as domestic testing capacity increased thereafter, private testing was beyond the jurisdiction of administrative testing; there was no coordination between the two. The shortage of test kits demanded a more detailed explanation.
Another issue is that no tracing was done for those who tested positive under private testing. This is a major difference from United Kingdom, Germany, and the United States. Due to the lack of tracing, the situation of community-acquired infections in Japan remains unknown, and the number of cases in Japan is thought to be lower than the true number of infections.
In light of this, the “COVID-19 AI Simulation Project Advisory Board” proposed a PCR monitoring test for asymptomatic people (12). The Office for Promotion of Countermeasures against Novel Coronavirus Infections, Cabinet Secretariat, spearheaded and implemented this proposal on a total of 1 million people in 14 prefectures where the state of emergency was declared during the third wave between February and October 2021. The results of the testing revealed a good correlation between the PCR test positivity rates of the asymptomatic general population and the number of cases, that it could be considered an indicator of community-acquired infections, and that the rate of false positives from the PCR test of asymptomatic people was extremely low (13-15). This project has been taken over by the prefectures this January, where free PCR testing for asymptomatic people is now being implemented across Japan. Interestingly, the PCR positivity rates for asymptomatic people during the peak of the fourth and fifth waves in Tokyo was about 0.3% (13-15), whereas the positivity rates for asymptomatic people during the peak of the sixth wave was 9% in Tokyo Metropolis and 8% in Shizuoka Prefecture – a good 30 times higher than in Tokyo Metropolis during the fifth wave (16, 17) (Figure 4, 5). This increase was likely because asymptomatic people deemed to be at a high risk for infection underwent free PCR testing, rather than just from an increase in the number of asymptomatic infected people in the sixth wave. Incidentally, a private testing company (F medical equipment Inc) that conducted saliva PCR tests on approximately 25,000 people who planned to participate in the Tokyo Marathon at the end of this February, stated that the PCR positivity rate was 0.55%. If the people who tested positive from the free PCR testing do not continue to undergo administrative testing, it would not only be difficult to determine the number of cases, but also to take appropriate measures for the symptomatic cases.
The PCR test positivity rate of asymptomatic people and Ct values of positive people are important indicators for understanding the situation of the community transmission. Yet only a limited number of local governments publish positivity rates. The national government should investigate the reasons why local governments are reluctant to publish such data, as well as gather these data and publish the results of subgroup analyses of age group, work place, region, and school, together with the primary data. The quality of test kits used in private testing, including antigen tests, and the accuracy of the tests themselves must also be controlled.
Performing PCR testing on public, regardless of the presence or absence of symptoms, is the cornerstone of COVID-19 measures. The purpose of performing PCR testing on asymptomatic people is not to conduct a census, but to investigate high-risk individuals and high-risk regions, and conduct sentinel surveillance and active surveillance. Based on this idea, public PCR testing should have been rolled out from the early pandemic phase, even if private testing resources have to be tapped into, and infection control measures should have been taken to include both symptomatic and asymptomatic people. Yet the information on PCR testing currently conducted on asymptomatic people is almost never published, with the exception of Tokyo Metropolis and Shizuoka Prefecture. It is clear that Japan’s response to asymptomatic carriers specified in the Infectious Diseases Control Law is inadequate. To balance infection control and socioeconomic activities, there is a need to expand public PCR testing as pointed out in the “Urgent recommendations on the expansion of PCR tests for COVID-19 infection control” of the Japan Medical Association COVID-19 Expert Meeting held in August 2020 (18).
 |
| Figure 4: Number of new patients (left) and PCR test positivity rate of asymptomatic people (right) during the sixth wave (January to April 2022) in Tokyo Metropolis. The number of new patients as well as the PCR test positivity rate of asymptomatic people are prepared by the author based on information respectively taken from https://stopcovid19.metro.tokyo.lg.jp/ and https://www.fukushihoken.metro.tokyo.lg.jp/iryo/kansen/kensa/kensuu.html. |
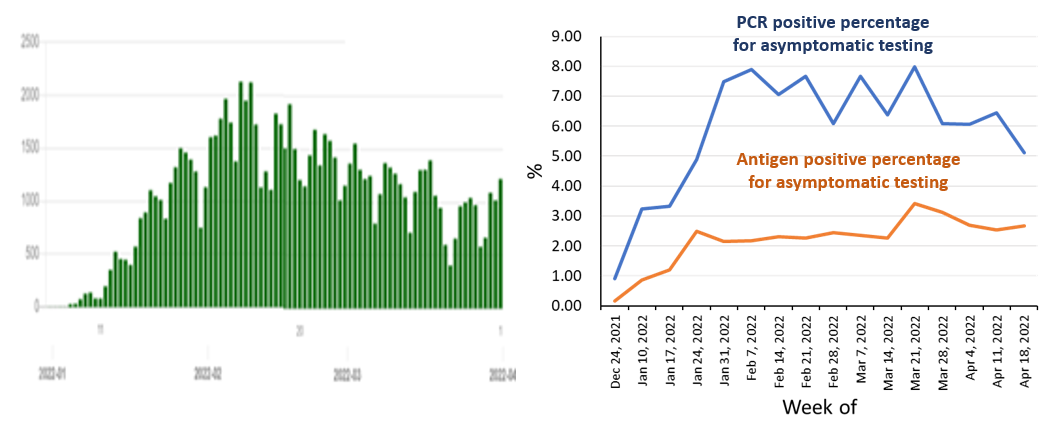 |
| Figure 5: Number of new cases (left); PCR test positivity rate and antigen test positivity rate of asymptomatic people (right) during the sixth wave (January to April 2022) in Shizuoka Prefecture. These are prepared by the author based on data published by Shizuoka Prefecture. Data on the number of cases as well as the PCR positivity rate and antigen positivity rate of asymptomatic people are respectively taken from https://stopcovid19.code4numazu.org/ and http://www2.pref.shizuoka.jp/all/kisha.nsf/c3db48f94231df2e4925714700049a4e/9141ca770a116430492588320011e1e4?OpenDocument. |
5) Legislation for major health crisis
In the interviews and discussions conducted to date in this expert meeting, many have opined that legislation should have been enacted from normal times to prepare for a pandemic. Despite the fact that the revisions of Infectious Diseases Control Law and the Special Measures Act last year have led to improvements, many difficulties in securing hospital beds and gathering of information still persist, and detailed arrangements are required to mitigate it. In addition, there is a need to clarify the chain of command between the national government, prefectural governors, ordinance-designated cities, and mayors of special wards and municipalities, so as to strengthen the coordination functions. This is not only a problem specific to the COVID-19 pandemic, but also to the state of the administrative authority of the government and local governments in crisis management. This pandemic has clearly demonstrated that the Infectious Diseases Control Law and Special Measures Act have to be revised in order to prepare a contingency healthcare system. Recent discussions in the government’s 33rd Local Government System Research Council, which commenced its activities this January, highlighted that contingency legislation covering healthcare is one of the main issues to be resolved. An important point brought up in the discussions was an appropriate governance structure sufficient to ensure public trust, and the sharing of information to explain to the public. Therefore, a system with a framework in place to gather information during a pandemic should be established as the topmost priority.
In this pandemic, physicians, nurses, and other healthcare professionals provided wide-area support through administrative communication and requests for cooperation from the ministries and agencies concerned. In the future, we should consider the dispatch of personnel from the national government and local governments according to the Basic Act on Disaster Management, as well as the enactment of legislation such as the Emergency Fire Rescue Team according to the Fire and Disaster Management Organization Act, based on the Guidelines for Emergency Response Activities, such as DMAT and DPAT that have proven track records in disaster-relief medical care.
2 Ideal state of expert advisory board
The advice of experts is important not only for the government to take infection control measures, but also to boost public acceptance through risk communication. In particular, the COVID-19 pandemic is a new experience for everyone where information gathering, investigations, research, and easy-to-understand explanations are imperative. However, the SARS-CoV-2 virus has continued to mutate, causing unexpected outbreaks even amongst experts. There are restrictions on the gathering of information, and the information published and explanations have not always been sufficient. Some have opined that the analyses of experts used to make policy decisions are also rarely publicized in detail and relied on limited mathematical models and analysis. It is important to ensure scientific validity and transparency through the publication of information and easy-to-understand explanations to the public.
In a national crisis such as a pandemic, interdisciplinary analysis and sharing of the latest findings are crucial. Expert advisory board must therefore analyze local and international epidemiological, clinical, and basic research information, as well as promote local investigations and research to establish concrete measures. They also need to collaborate with various researchers, and at the same time, clarify the basis and positioning of expert advisory board and their involvement with other meetings. The members will include as many professionals with research experience as possible; the addition of clinical researchers and immunologists will enable a system that can provide guidance in interdisciplinary analysis and clinical research. There should also be two sides to the expert advisory board as they deal with the government: cooperative and demanding. If there is insufficient information, it is our responsibility as scientists to gather information and provide recommendations, advice, and requests for cooperation to the government, local governments, and the public so as to promote research in Japan.
1) Issues with PCR testing
I have talked about the ideal state of PCR testing (see page 11-13). This issue needs to be discussed not only by those involved in public health, but also by the scientific societies of laboratory medicine and clinical medicine in the future.
At the beginning of the pandemic, the main reason why PCR testing could not be expanded was the lack of testing reagents, which had to be explained to the public. Other than that, there were also concerns about false positives in the tests, to which the Subcommittee on Novel Coronavirus Disease Control explained its policy of assuming a false positive rate of 0.1% for PCR testing in October 2020 (19). If the false positive rate is assumed to be 0.1%, then the positive predictive rate for determining infected cases will be 41% when PCR testing is performed simultaneously in a population with an infection rate of 0.1%. This, combined with the lack of test kits, was the reason why PCR testing was prioritized for infected cases and their close contacts (19).
It is not easy to obtain data showing the false positive rates for PCR tests, but PCR test positivity rates of asymptomatic people when the outbreaks subsided can be helpful. To put it in numbers, the Office for Promotion of Countermeasures against Novel Coronavirus Infections, Cabinet Secretariat conducted PCR testing on 50,220 asymptomatic people between June 28 and July 4, 2021 – the trough between the fourth and fifth waves – and found that 14 (0.028%) of them were positive (Reference material (15); Figure & Table 9). Further, the Tokyo Metropolis conducted free PCR testing on 8018 people right before the sixth wave, from last December 20 to 26, an found zero positives (16). These data suggest that the false positive rate of the PCR test is much lower than the 0.1% assumed, and the positive predictive rate is higher than 41%. If this is the case, rather than narrowing down the target population based on prior probabilities, we should consider a testing strategy that expands the testing capacity to include surveys in high-risk regions and populations, surveillance of the general population, and a wider range of people who need to be tested for socioeconomic activities. This is why it is necessary to control the accuracy of the PCR test and explicitly specify the Ct values to be used in the interpretation of positive test results. Test kits could be secured if we cooperated with private testing.
The policy for testing COVID-19 between border measures and community-acquired infection control measures is different. There is a need to balance both socioeconomic activities and infection control especially after the summer of 2020. To achieve this balance, we need to have a firm grasp of the false positive rate of the test, and employ PCR testing in surveillance and other purposes to understand the situation of the community-acquired infections. Experts are responsible for giving advice on the revision of the testing system in response to the situation of the outbreak and socioeconomic changes.
2) Issues surrounding counter-cluster measures and active epidemiological investigation
Responding to clusters that occur in hospitals and student dormitories is the cornerstone of infection control, and some effectiveness has been observed in the community during the early pandemic phase (20). The expert meeting advocated the importance of counter-cluster measures based on the observations of 110 people in the early pandemic phase, and contributed to raising social awareness such as “Avoid the Three Cs” (21). At the same time, the expert meeting also explained that “80% of the infected cases do not infect others, but the remaining 20% will create cluster of infections that will spread, and the outbreak can be contained to some extent by controlling the clusters”, and promoted “retrospective contact tracing” to trace the source of infection back to the first patient (22, 23).
But in a situation of widespread community-acquired infections, scientific verification is required to determine how effective “retrospective contact tracing” was in preventing the spread of infection in the region in future. In fact, according to the Tokyo Metropolis data from April 2020, the rate of cases with unknown infection route accounted for about 70 to 80% of infected cases, and remained at 60 to 70% thereafter (24). This simply means that even if COVID-19 were to expand into the region around a cluster, it is impossible to capture all clusters.
This is why it is necessary to take measures to prevent the next wave of outbreak by promoting counter-cluster measures as well as employing surveillance, to which a balance between the two is important. There are limits to the functions of Public Health Centers. If we are unable to understand the situation of community-acquired infections because of an overemphasis on “retrospective contact tracing”, then we need to review the system. Even though “retrospective contact tracing” has not been performed in Tokyo Metropolis since last August due to the spread of community-acquired infections, it is still considered effective in preventing the spread of infection in Tottori Prefecture where the infection rate was low (25). It is therefore important to respond in a detailed manner and provide explanations rather than implementing a uniform policy nationwide. Experts need to hold multifaceted discussions on how “active epidemiological investigation” and “retrospective contact tracing” should be done to handle the changes in the situation of infection.
The duty of the expert advisory board is to engage in open-ended discussions during crisis management and provide appropriate scientific advice as the situation changes. It is therefore important for expert advisory board to clarify their positions and their involvement with other meetings, and to recruit a diverse workforce who can think out of the box (26). In other words, we should form a consultative body that coordinates with other academic societies, and establish a data center that operates in collaboration with academia to publish data widely, especially during a pandemic.
3 Issues with research systems
In 2020, the Center for Research and Development Strategy, Japan Science and Technology Agency (JST-CRDS) compiled a report on the recommendations for the establishment of an infectious diseases research platform in preparation for pandemics (27). In any research institution, it is crucial that research is conducted in a non-hierarchical structure environment that is open to new ideas and encourages cross-disciplinary personnel exchange. Especially in an unprecedented situation of a pandemic caused by a new virus, we must deal with the situation by conducting investigations and research with a flexible mindset.
Japan has released few reports on COVID-19 in this pandemic, and is ranked 16th in the world for the number of papers published in 2020. The scientific advisory system has deteriorated under this situation. Nonetheless, the number of papers and ranking of Japan began to improve, achieving 14th in 2021 and 12th in 2022 (Figure 6). This might have been due to the difficulty in providing data to researchers during the early phase of the pandemic. Other reasons include a lack of a system to gather the essential epidemiological information, a weak system for broad discussions in academia, a lack of a clinical research system at core hospitals to evaluate the efficacy of therapeutic drugs and vaccines, and little experience in international joint research. There is a need to establish a clinical research system from normal times, as well as develop a system for mobilizing researchers and research resources in times of pandemic.
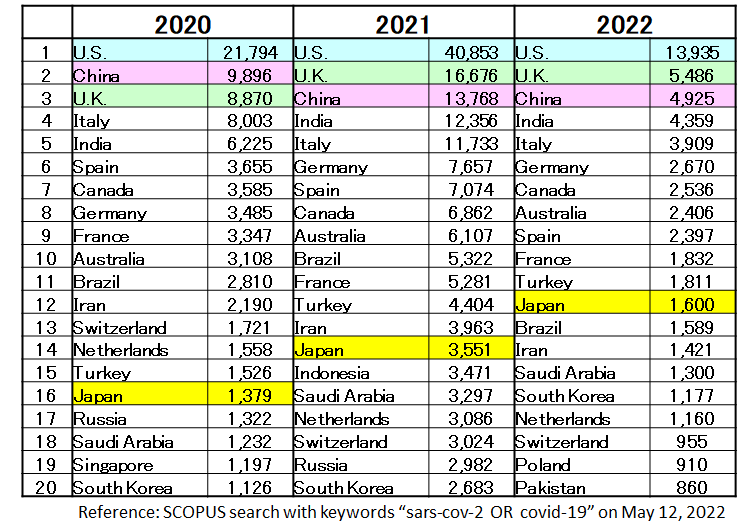 |
| Figure 6: A comparison of the number of papers on COVID-19 published by countries in the world (2020 to 2022). Japan gradually moved up the rankings, from 16th place to 14th place, and finally to 12th place. Japanese researchers might not have had access to data at the beginning of the pandemic. Prepared by Fellow Masahiro Tsuji, Center for Research and Development Strategy, Japan Science and Technology Agency (JST-CRDS). |
A critical issue is the situation of basic research in Japan. The rapid development of therapeutic drugs and vaccines in other countries was driven by foreign researchers who unceasingly investigated the coronaviruses from a scientific point of view, such as the mechanisms of infection of coronaviruses across animal species, genome replication mechanisms, genome mutation and evolution, and RNA engineering. Moderna was originally developing an mRNA vaccine for MERS based on their past experience with coronavirus infections and their research infrastructure. But when the Chinese authorities released the genomic sequence of COVID-19, they changed their plans and started manufacturing the COVID-19 vaccine three days later, on January 13, 2020 (28).
Japan’s research budget for infectious diseases is overwhelmingly small compared to other fields (Figure 7). In addition, AMED’s research funding for infectious diseases is focused on practical research, such as the development of vaccines and drugs, and do not support large-scale basic research. To make matters worse, it is difficult for AMED to use its discretion beyond the intentions of the ministries from which it receives its budget. The Ministry of Health, Labour and Welfare also provides and directly manages the research funding for infectious diseases, but at JPY 2 billion (as of 2020), it is relatively small even among major countries. Although the Ministry of Education, Culture, Sports, Science and Technology provides Grants-in-Aid for Scientific Research (KAKENHI), the funding is mainly for small-scale research, with the exception of a few large-scale basic research projects on infectious diseases.
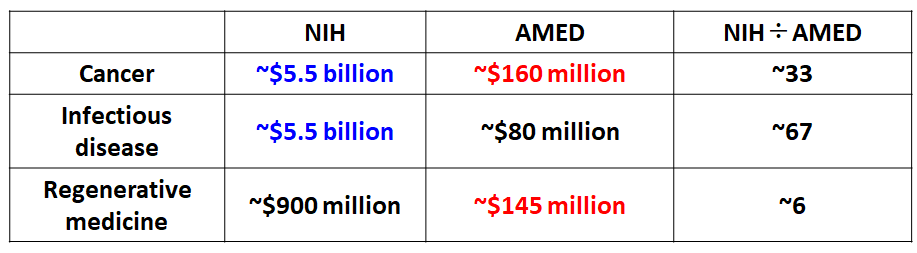 |
| Figure 7: A comparison of R&D budgets for medical care in Japan and the United States (annual average budget for 2016 to 2019 before the COVID-19 pandemic). The United States places equal emphasis on cancer and infectious diseases, whereas Japan allocates very little budget to R&D on infectious diseases. Prepared by Fellow Masahiro Tsuji, Center for Research and Development Strategy, Japan Science and Technology Agency (JST-CRDS). |
Emerging and re-emerging infectious diseases that have spread to human society are often the result of zoonotic spillover due to climate change, natural destruction, and globalization. There are also reports warning of a significant increase in the risk of pandemics due to climate change (29). It is impossible to predict which virus will cause the next pandemic. This is why international collaborative research with overseas infectious disease hot spots is essential (27). After the SARS crisis, the Ministry of Education, Culture, Sports, Science and Technology in Japan launched the Program of Founding Research Centers for Emerging and Reemerging Infectious Diseases. This has led to joint research with China and promoted personnel exchange between the two countries. This exchange has proven to be fruitful in terms of sharing of information in this pandemic as well. But cuts in research budgets in the recent years coupled with an increase in the number of research centers have led to a drastic decline in research funding for the program (Figure 8). Even the budget and personnel of the National Institute of Infectious Diseases were weaker than that in major countries when the pandemic happened (Figure 9) (27).
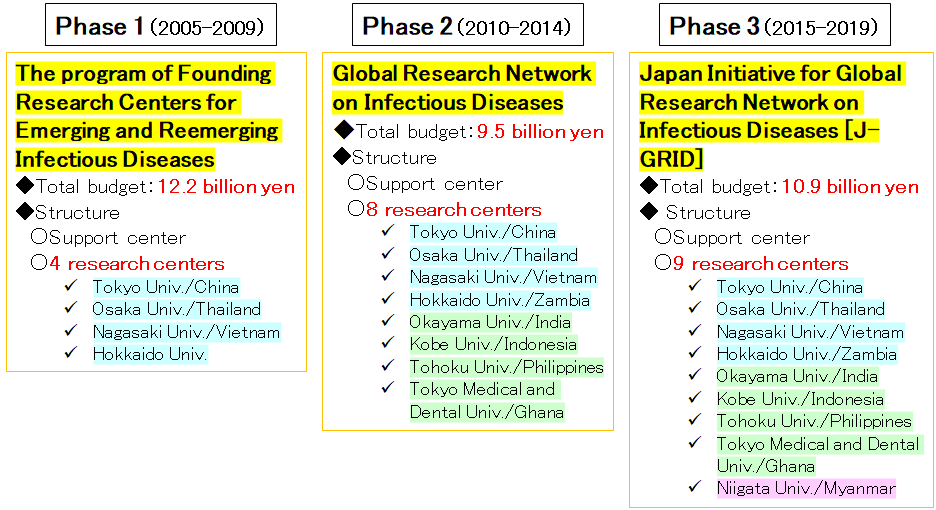 |
| Figure 8: International joint research projects and budgets for infectious diseases by the Ministry of Education, Culture, Sports, Science and Technology. Although the budgets for international joint research projects on infectious diseases are declining, the number of adopted projects more than doubled, resulting in a significant decrease in the size of the budget for individual projects. Prepared by Fellow Masahiro Tsuji, Center for Research and Development Strategy, Japan Science and Technology Agency (JST-CRDS). |
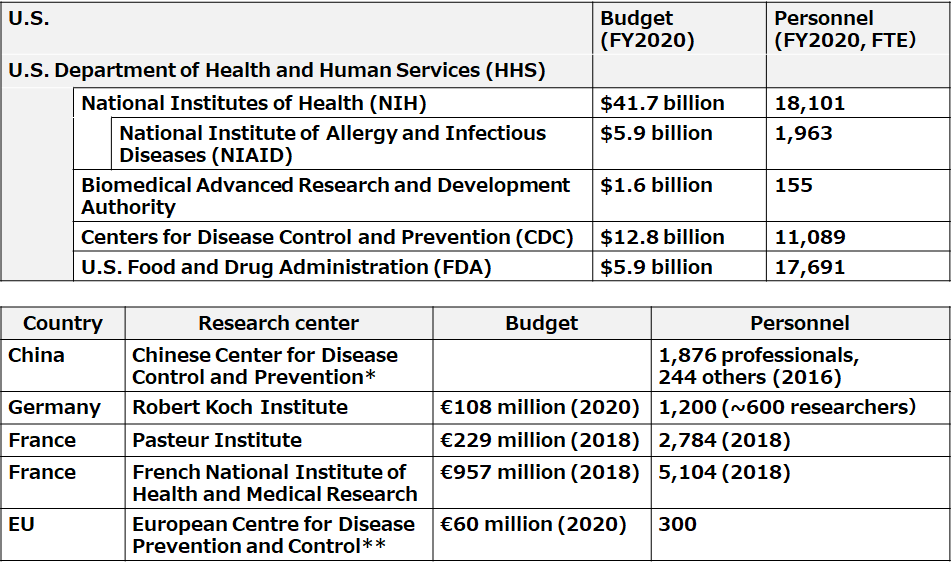 |
| Figure 9: Budgets and staffing in research institutions for infectious diseases and agencies for disease control in major countries during the COVID-19 pandemic outbreak. Figures for the National Institute of Infectious Diseases are as of 2020. In 2021, the number of employees was increased to 716. Based on materials from the Center for Research and Development Strategy, Japan Science and Technology Agency (JST-CRDS). |
There are also many issues regarding the utilization of specimens from infected cases. In the spring of 2021, when COVID-19 variants became a concern, the genomic data of the variants was integrated with the clinical information of infected cases, which led to a discussion of various issues such as the risks of developing severe complications, treatment effects, and vaccine efficacy against the variants, as well as the utilization of specimens in developing therapeutic drugs and vaccines while addressing public health issues. However, there were many obstacles to moving forward with the plan due to the insufficient capacity of the National Institute of Infectious Diseases, the lack of a common data platform that researchers in academia can access to, and restrictions on obtaining consent from the busy clinical sites. We need to take this opportunity to develop and establish a system for the utilization and provision of specimens to third parties during a pandemic that will bring about a major health crisis.
4 Issues with the infrastructure and presentation of information
In a pandemic, the situation can change rapidly. A centralized data center needs to be established to develop measures that will offer us a bird’s eye view of the entire situation. It is extremely important for us to consider the design of the data center from normal times – it should have a system capable of agile and flexible analysis, where researchers can share data with the society, as well as a data structure that enables the combination and analysis of diverse data based on the assumptions that the data will be used by researchers in various specialties. In addition, the necessary legislations, the agencies in charge, and the format must be prepared in advance from normal times. It is also crucial to utilize interdisciplinary human resources and to explain to the public in an easy-to-understand manner using the data (risk communication).
Digital reforms have been slow to take off at the point of care, despite the flood of various information from normal times. A large number of small medical institutions continue to use facsimile for their communications with the Public Health Centers regarding infected cases simply because they do not have access to the Internet (30). The information infrastructure of Public Health Centers and related administrative organs are also severely lagging behind. There are also many other issues concerning the sharing of information and operational efficiency in the COVID-19 pandemic (31). The patient registration system, HER-SYS, also has many problems with duplicate registration, as well as data entry burden according to Article 15 of the Infectious Diseases Control Law, security, and system design (30). In addition, the COVID-19 contract tracing application, COCOA, has only a few users; it is unclear how well it worked (32). One of the reasons why so many failures occurred in the system of coronavirus measures is that the application was not created from the user’s perspective by referring to the opinions of those who understand the point of care well. It is important to discuss with the relevant parties prior to developing an application; if nothing else, it should never be left up to the vendor.
Improvements are also required in the data publication by the national government and local governments. Take for instance the publication of HER-SYS data – administrative organs and the researchers of the National Institute of Infectious Diseases may handle it, but not the researchers in the private sector. The data should be made available after processing, such as anonymization. Information on the side effects of vaccines is also scarce compared to Europe and the United States. The Cabinet Secretariat, Ministry of Health, Labour and Welfare, and local governments publish their data in their own way, which is inconsistent. Most of the data are still published in pdf format. In addition, only one week’s worth of new data was published, and previous weekly data was often erased. Unless screenshots of the data were taken weekly, it was impossible to analyze changes over time. Even the data on the number of cases by age group in Figure 2 was published for the most recent week only until the end of last year, and previous data was simply incorporated into the cumulative total. The infection rates for each group could be calculated because we could combine the recently published primary data with the population by age group. In a pandemic, data files should be published so that researchers can use the data for secondary purposes or analyses.
There are many issues with how the information was communicated to the public as well. It is important to strive to “publish easy-to-understand information” for foreign nationals in Japan and abroad as well.
5 Ideal state of command center
Based on the discussion thus far, it is clear that there is a need to strengthen the functions of the government’s command center. The command center needs to ensure 1) transparency, and 2) scientific excellence (human resources), as well as put in place the various environments described in this written opinion. Cooperation with the Deputy Chief Cabinet Secretary for Crisis Management is especially crucial during a state of emergency. Additionally, a two-pronged approach should be adopted, in which the “command center is responsible for explaining the measures” while the “expert advisory board are responsible for providing support from a scientific perspective”.
In this context, the recommendations made by the “Committee on the Establishment of the Japan CDC (tentative name) (2nd round)” (chaired by Professor Hiroyasu Iso, Osaka University) established by the Japanese Medical Science Federation, will be helpful (33). Simply put, the Committee proposes the following “in order to make policy recommendations based on scientific evidence”: comprehensive collection, analysis, accumulation, and publication of information on health crises; provision of evidence that will facilitate operations in a state of emergency; provision of information to support the generation of evidence in academia; collection, analysis, accumulation of information through collaborations with international agencies and overseas research institutions, and transmission of information overseas; support for the development and utilization of human resources capable of responding to health crisis management; and the creation of a permanent organization aimed at the extensive disease control and prevention over the medium to long-term. On the other hand, the Committee also advocates for “this permanent organization to provide technical and personnel support for operations in a state of emergency and operational departments, especially the government, while maintaining its functions, in the event of critical situations”. Further, the Committee recommended policies, such as the “sharing and utilization of necessary information among the national government, local governments, academia, and the public through centralization of information into one common repository”; “utilization of information and samples to promote the generation of evidence in academia”; “strengthening of cooperation and collaboration between the national government, prefectures, municipalities, ordinance-designated cities, and special wards from normal times”; “radical review of the healthcare system in response to health crisis management”; and “guarantee surge capacity through human resource development during normal times and emergency mobilization”. These recommendations should be used in conjunction with the Scientific Advisory Group for Emergencies (SAGE) in United Kingdom, New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG), and Scientific Pandemic Influenza Group on Modelling (SPI-M) as a reference in future discussions (34).
Conclusion
The number of COVID-19 cases and number of fatalities in Japan are lower than that in major countries, and the measures appear to be successful. However, some have pointed out the low numbers of PCR testing, the inadequate understanding of the actual situation of community-acquired infections, and that the Japan model, that is, request-based measures instead of compulsory ones, made it difficult to make prompt decisions. The Japanese public is skeptical of how the government has handled this pandemic. It is of particular concern that there is no sharing of the scientific lessons that can be used for the next pandemic. The burden placed on the point of care as well as the significant social, economic, and financial burdens that arose from the coronavirus measures deserve attention as well. One could also say that the widening educational and economic disparities, declining marriages, declining fertility rates, and isolation of students due to the normalization of remote classes are complications resulting from the coronavirus measures. Thus, infection rate and severity of COVID-19 disease, and the impact of the infection control measures on daily life vary greatly from generation to generation. It is therefore important to listen to the opinions of various generations when formulating measures.
Coronaviruses have gained attention as zoonotic diseases due to the SARS outbreak in 2003 and the MERS outbreak in 2012. Studies on the viral mutations of the coronaviruses have however suggested that the Russian flu of 1890 may also have been a coronavirus infection (28, 35). In addition, the respiratory plague in the Song Dynasty in the 11th century, and pneumonia of unknown cause in an abandoned mine in Tongguan town, Yunnan Province, China in 2012, have also attracted attention (28). It is clear that various zoonotic diseases, including coronaviruses, will continue to cause pandemics (29). There is a pressing need to develop legislations, create systems, and boost research capabilities for public health contingencies from normal times. The fundamentals of pandemic measures are to gather the necessary information from the necessary locations using multiple methods and distribute the burden. It is also important that the measures be a combination of multiple methods instead of a single one. We should review the functions of the command center since these have not always been done in Japan. But given Japan’s negative history with the Infectious Diseases Control Law, there is a need to have a deep debate concerning the ideal state of governance and governance institutions for establishing laws and strengthening the functions of the command center. For the sake of discussion, it is desirable to thoroughly review how the information should be gathered during the pandemic, ideal state of data centers, data utilization, and the ideal way to go about publishing information during the pandemic.
This pandemic is a new experience for everyone and errors in judgment are inevitable. It is important not to point fingers at each other, but to respond to the situation in a flexible manner, do all in our power at that time, and explain the situation and policies to the public in an easy-to-understand manner.
The debate over COVID-19 disease control and prevention measures is not limited to the issues surfaced in the infection control measures and crisis management in Japan. It is also a question of how to control and come to terms with complex phenomena that cannot be handled by rationalism alone. It includes information infrastructure, data centers during the state of emergency, data-driven thinking, analysis and predictions, information sharing, information publication, accountability, social disparities, reputational damage, mutual aid and mutual assistance, as well as scientific advice and the ideal state of scientific research, and wisdom, technology, and other issues that should be resolved to survive in uncertain times. We hope that these will be continuously and multilaterally examined from various perspectives and situations in the future.
Reference (United Kingdom’s response)
Toru Suzuki, Professor/Chair of Cardiovascular Medicine, University of Leicester; Associate Dean of College of Life Sciences, University of Leicester; Project Professor, Institute of Medical Science, University of Tokyo
1 Issues with the laws regarding COVID-19 pandemic measures and administrative response
The United Kingdom passed the Coronavirus Act 2020 (https://en.wikipedia.org/wiki/Coronavirus_Act_2020) in March 2020 and took emergency measures, including lockdowns, in accordance with the Act. The National Health Service (NHS) moved systematically and quickly to secure beds in a top-down manner based on the results of their modeling (an instance would include the temporary Nightingale hospitals that were set up in April 2020). The focus was placed on the reorganization of the NHS (to free up around a total of 30,000 of its general and acute hospital beds, and set up field hospitals with a total of 20,000 beds) and the securing of medical resources (including 30,000 ventilators, personal protective equipment, development of diagnostic tests). There was an acute shortage of personal protective equipment.
When the pandemic first broke out and until the middle of March 2020, the United Kingdom responded with policies to contain, delay, mitigate the outbreak, as well as contact tracing. They were also expecting herd immunity to build in the general population. Yet in the very same year, they expressed apprehensions that their public healthcare system, NHS, would be overwhelmed, based on the modeling results (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-9-impact-of-npis-on-covid-19) published on March 16. To stop the outbreak, they abruptly changed the policies and declared a nationwide lockdown on March 23 as they aimed to suppress the spread instead. Ever since then, the Prime Minister, Chief Scientific Officer/CSO, Chief Medical Officer/CMO, and other officials have provided information to the public almost every night through the country’s national broadcaster BBC, and released the data and materials on which the announcements were based at about the same time.
The United Kingdom has allowed community-acquired infections within a certain range after the lockdown was lifted. They have monitored the progress of the outbreak based on the several criteria, including controlling the number of critically ill patients and fatalities, ensuring that any increase in hospital admissions must not lead to a shortage of hospital beds, promoting vaccinations, and that the emergence of new variants must not change the status quo.
The government controlled all testing, including PCR tests as well as LFT (lateral flow test, a rapid antigen test), and provided them free of charge to the public. At its peak, about a million tests were performed each day. The United Kingdom set up mega PCR laboratories called “Lighthouse laboratories”, which are centrally managed throughout the country. Swabs are sent to these laboratories by mail, drive-through and walk-through testing centers. They provided testing not only for people with symptoms, but also their close contacts. They also provided asymptomatic testing since about one in three cases of asymptomatic carriers, which is characteristic of the coronavirus infection, is infectious. They also provided LFTs to the general public so that individuals without any symptoms can take the rapid test twice a week at home or at work. In addition to this, they conducted door-to-door testing of all residents in areas where infection was widespread. In this way, they set up a testing system and strove to understand the actual situation of infection. Furthermore, they conducted genomic analysis on PCR samples and provided information on the emergence and tracking of variants to the rest of the world through the activities of COG-UK (COVID-19 Genomics UK Consortium) and others.
The Public Health England (PHE) was transferred into a new organization called the UK Health Security Agency (UKHSA) in March 2021. The UKHSA is an executive agency of the Department of Health and Social Care (“DHSC”; United Kingdom’s equivalent of Ministry of Health, Labour and Welfare), and its main responsibilities include public health protection and responding to infectious diseases. Under the direct control of the Secretary of State for Health and Social Care, the UKHSA is a single leadership structure that integrates the following five functions in order to eliminate the silo organizational structure seen in the country’s response to the COVID-19 pandemic and to further strengthen the organization.
・Test and trace function of NHS
・Function of the Joint Biosecurity Centre (formerly the health crisis management organization)
・Health protection functions and infection control measures by the Public Health England
・Planning and executing the response to external health threats such as pandemics
・Regulation of coronavirus diagnostic devices
2 Ideal state of expert advisory board
At the top of the chain of command is the DHSC, where branches of Public Health England (currently the UK Health Security Agency (UKHSA)) under its jurisdiction are responsible for gathering information from the local governments and conveying it back to the DHSC, thus consolidating the information control and operations. The data gathered is published daily on the government’s homepage (https://coronavirus.data.gov.uk).
In addition, expert groups such as the Scientific Advisory Group for Emergencies (SAGE) provided advice to the government at a Cabinet Office level (Cabinet Office Briefing Room, COBR). Under SAGE are New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG), an expert group on respiratory diseases, as well as Scientific Pandemic Influenza Group on Modelling (SPI-M), an expert group on modeling, to which their committees comprise members from the academia.
3 Issues with research systems
The United Kingdom has promoted the implementation of clinical trials and support systems, of which many clinical trials have been conducted by the NIHR (National Institute for Health and Care Research). The representative RECOVERY trial is known as the landmark trial that recruited 10,000 patients in the first three months after its commencement and demonstrated the efficacies of the drugs. Specifically, the first patient was enrolled into the RECOVERY trial on March 19, 2020 after it was awarded funding on March 3, 2020. On June 6, the results of an analysis of 10,000 patients demonstrated the efficacy of a steroid (dexamethasone). University stakeholders and healthcare professionals collaborated at the national level. It should also be noted that the United Kingdom moved quickly to introduce and secure vaccines. The United Kingdom invested in the securing (up-front investments) and development of vaccines, as well as providing them to the public in a timely manner.
NIHR is the research arm of NHS, United Kingdom’s public healthcare system. The NIHR is headed by the CMO, Professor Chris Whitty. The NIHR allocates budgets to NHS hospitals in the United Kingdom and oversees their operations (through organizations such as NIHR Biomedical Research Centre and Clinical Research Network). A noteworthy mention is that the NIHR was able to cope with this pandemic by promptly conducting epidemiological and clinical research through its nationwide collaboration setup (such as the clinical research that the NIHR has managed from normal times) and organizational infrastructure. There are no agencies in Japan that are equivalent to the NIHR in the United Kingdom.
Reference (Germany’s response)
Hisaki Makimoto, Associate Professor, Division of Cardiology, Heinrich-Heine University, Düsseldorf
Germany’s coronavirus measures have demonstrated the strength, agility, and flexible leadership of the federal government, especially in the acute phase of the pandemic in the beginning. As the pandemic prolonged, the local governments in each state took on more governance while the federal government continues to control the disease in the background.
1 Legal and administrative situations
The main legal basis for coronavirus measures is the Verordnungen (Ordinances). The regulations are enacted and promulgated by administrative organs in a faster and more flexible manner than laws (Gesetz) and are legally binding on citizens. The details of the regulations conform to the Verordnungen established by the federal government, and each state promulgates its own Verordnungen. Numerous Verordnungen have been promptly and frequently promulgated and revised according to the situation of infection. The Protection against Infection Act (Infektionsschutzgesetz, IfSG) has been around for some time, but it was mainly used for the reporting of specific dangerous communicable diseases. The IfSG has been substantially revised in light of the pandemic, and is still in force with repeated revisions. Take for instance the revision of IfSG in April 2021 – A system of lockdowns to be imposed or lifted automatically based on the number of new cases per 100,000 residents would be implemented across Germany.
Both public and private hospital facilities have always under the control of administrative organs from normal times. This was why requests from the administrative organs to secure hospital beds during the first wave of infection, for instance, could be promptly and thoroughly implemented.
2 Experts’ opinions, reflections on policy
Since the early phase of the pandemic, the federal government has consistently relied on the advice of the Robert Koch Institute (RKI) to decide the measures to be taken. The RKI is committed to gather and publish information not only for the government but for the general public as well. During the acute phase, the RKI also held daily press conferences to explain the various information flying around from a scientific point of view. They would publish the gathered information quickly on their homepage. Although the opinions of RKI were not always 100% reflected in the policies, it utilized a structure that was easy for the public to understand.
3 Research systems
It is not common for the public health administrative organizations to collaborate with the research institutions to support COVID-19 research, for example by providing data. The backdrop to this is that the RKI, a government agency, is presumably already largely responsible for public health research as its primary mission. The RKI publicly collects all data related to infectious diseases. To date, the RKI has published over 250 papers on COVID-19.
In terms of research funding, the administrative organs have actively supported COVID-19 research since the pandemic first broke out. The Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung) has set aside a budget of up to €45 million in funds for COVID-19 research over a two-year period until 2022, which has supported about 25 independent and joint research projects thus far. Deutsche Forschungsgemeinschaft (DFG), Germany’s equivalent of the Japan Society for the Promotion of Science, has been conducting joint research with China since the beginning of the pandemic, and spent €3.6 million to research on COVID-19 in 2020 alone.
(Reference: BMBF homepage https://www.gesundheitsforschung-bmbf.de/de/erforschung-von-covid-19-im-zuge-des-ausbruchs-von-sars-cov-2-11483.php, DFG Annual Report 2020 http://83.143.2.157/download/pdf/dfg_im_profil/geschaeftsstelle/publikationen/dfg_jb2020.pdf)
4 Information infrastructure and information publication
The state health ministries collected information on new infections and the situation of bed shortages, and promptly communicated it back to the Federal Ministry of Health (Bundesministerium für Gesundheit). The RKI has compiled and published such information from the beginning. They publish daily updated information such as the number of new cases and fatalities, and the PCR test positivity rates, on its website.
Germany also launched Corona-Warn, a contract tracing application, but no instances of its proactive use has been seen or heard. It remains unclear how well it worked.
Germany not only oversees PCR testing, but the results as well. The ordinances (Verordnungen) that are in place to control quality and monitor results of COVID-19 testing, are frequently revised as testing methods evolve. The designated testing agencies, regardless of public or private, are obliged to report the PCR test results, even if it is not medically necessary.
Germany has created objective indices to show the spread of infection and has used them as a basis for imposing restrictions on the lives of her citizens. All of these are indicators that strongly emphasize a sense of distance to the collapse of healthcare. In the early phase of the pandemic, the reproduction number (Reproduktionszahl, “R-value”) was used. It is an indicator of the average number of secondary infections produced by a single infected person. This R-value was used to urge the public to continue to be prudent when the government decided to ease the lockdown in the first wave. The public was given explanations like, “If the R-value exceeds 1.1 based on the total number of hospital beds in Germany, our healthcare system will collapse in six months”. After that, Germany started to use “7-Tage-Inzidenz” to refer to the number of new cases recorded per 100,000 residents in the past seven days. In April 2021, when vaccinations were not widespread, Germany established a rule that if the 7-Tage-Inzidenz exceeded 100 for three consecutive days, the so-called lockdown would automatically be imposed from the day after that. This rule has been suspended since the summer of 2021 in light of the changes in the situation as more and more residents got vaccinated, and a bed shortage would not occur even if the 7-Tage-Inzidenz exceeded 100. After the fall of 2021, the emergence of the Omicron variant led to an explosive increase in the number of new cases, and the number of Inzidenz (new cases) continued to rocket to 1000-2000 throughout Germany during the winter season. Although this resulted in acute bed shortages, the healthcare system did not collapse and no lockdowns were imposed. Even now, there are almost no regions with a 7-Tage-Inzidenz under 100. Germany therefore introduced “7-Tage-Hospitalisierungsinzidenz” – a new value referring to the number of new hospital admissions due to COVID-19 per 100,000 residents in seven days. However, this indicator has become a problematic one due to its large time lag and omissions in reporting. When a shortage of beds starts to occur, Germany may very likely create new indicators again.
5 Ideal state of command center
Looking back on the first two years of the COVID-19 pandemic, it appears that Germany’s politicians and infectious disease experts have demonstrated their leadership in a good way. This may be due to several factors such as their RKI, which was originally a government agency primarily responsible for conducting research on infectious disease and public health; a strong chain of command over the medical institutions (including private ones), from the states and, by extension, the Federal Ministry of Health; a robust information management and publication system; and that Germany’s economic situation is strong enough to provide compensation associated with the coronavirus policies. During the first two years, scientists presented the latest information and their interpretations, to which the politicians based their own political decisions on, and implemented them under their own responsibilities. As a result, administrative organs were able to respond quickly to the changes in the situation. Instead of holding long discussions aiming for perfection, they have been quick to push out policies that seemed reasonable at least, quickly correct them if they were not, and the citizens have come to accept this. Although various factors such as national character, culture, and religious views come into play, Germany’s positive attitude in combating the coronavirus and doing everything in her power without fear of making mistakes since everyone makes mistakes and no one knows what will happen in future, may serve as a good reference on how a command center should be.
Reference
- Koji Wada, Tatsuo Miyamura (supervision), Novel influenza (A/H1N1) – Responses and future issues in Japan, Chuo-hoki Publishing Co., Ltd., 2011
- Nick Triggle, Covid: UK’s early response worst public health failure ever, MPs say
BBC News, https://www.bbc.com/news/health-58876089, 2021.10.21 - Neil M. Vora, Lee Hannah, Susan Lieberman, Mariana M. Vale, Raina K. Plowright, Aaron S. Bernstein, Want to prevent pandemics? Stop spillovers, Nature 605: 419-422,2022,
https://www.nature.com/articles/d41586-022-01312-y, 19 May 2022 - David Michaels, Ezekiel J. Emanuel, Rick A. Bright, A National Strategy for COVID-19: Testing, Surveillance, and Mitigation Strategies,
JAMA 2022; 327: 213-214. doi:10.1001/jama.2021.24168 - Yuri Okina, What Can We Learn from Germany’s Response to COVID-19? – Medical Preparedness / Flexible Responses / Management of Public Funds – NIRA Opinion Paper No. 54, 2020.10.30
https://www.nira.or.jp/paper/opinion-paper/2020/post-14.html - House of Commons Health and Social Care, and Science and Technology Committees,
Coronavirus: lessons learned to date, Sixth Report of the Health and Social Care Committee and Third Report of the Science and Technology Committee of Session 2021–22
https://committees.parliament.uk/publications/7496/documents/78687/default/ - Asia Pacific Initiative, The Independent Investigation Commission on the Japanese Government’s Response to COVID-19: Report on Best Practices and Lessons Learned, Discover 21, 2020
- Kiyosu Taniguchi, Indications for PCR and other COVID-19 nucleic acid amplification testing (NAAT) from a surveillance perspective, Japan Medical Association COVID-19 Expert Meeting, https://www.covid19-jma-medical-expert-meeting.jp/topic/4539, 2020.5.13
- Kiyosu Taniguchi, Yoshito Iwade, Assessing the risk of COVID-19 in the community by sentinel surveillance of coronavirus-like diseases, Takemi-Fund COVID-19 Expert Meeting, https://www.covid19-jma-medical-expert-meeting.jp/topic/6809, 2021.7.30
- Naomi Seki, Public Health Centers’ “Account of the War Against the Coronavirus” Tokyo 2020-2021, Kobunsha Co., Ltd., 2021
- Katsuhiko Uchida, Strengthening of the Public Health Center’s crisis management system of infectious diseases – including issues with COVID-19 measures, The Journal of Public Health Practice 85, 751-756, 2021
- The 3rd Meeting of the AI Advisory Board, https://corona.go.jp/prevention/pdf/advisory_siryou_20201026.pdf, 2020.10.26
- Kenichi Aizawa, Toru Suzuki, Kenji Shibuya, Shinya Yamanaka, Yuichiro Anzai, Kiyoshi Kurokawa, Ryozo Nagai, Asymptomatic infection of SARS-CoV-2 in Japan, in submission
- Ryozo Nagai, Kenichi Aizawa, Significance of COVID-19 monitoring test of the general population with saliva PCR (1), Takemi-Fund COVID-19 Expert Meeting, https://www.covid19-jma-medical-expert-meeting.jp/topic/6570, 2021.6.28
- Ryozo Nagai, Kenichi Aizawa, Significance of COVID-19 monitoring test (2): Changes after the delta variant, Takemi-Fund COVID-19 Expert Meeting, https://www.covid19-jma-medical-expert-meeting.jp/topic/6954, 2021.9.3
- Data on the number of tests conducted by Tokyo Metropolitan Government, Bureau of Social Welfare and Public Health, Tokyo Metropolitan Government, https://www.fukushihoken.metro.tokyo.lg.jp/iryo/kansen/kensa/kensuu.html
- Materials provided for the press by Shizuoka Prefecture, Shizuoka Prefecture official homepage, http://www2.pref.shizuoka.jp/all/kisha.nsf/c3db48f94231df2e4925714700049a4e/9141ca770a116430492588320011e1e4?OpenDocument
- Japan Medical Association COVID-19 Expert Meeting, Urgent recommendations on the expansion of PCR tests for COVID-19 infection control, https://www.covid19-jma-medical-expert-meeting.jp/topic/3243, 2020.8.5
- Subcommittee on Novel Coronavirus Disease Control, Basic strategy and thoughts on testing system (2nd edition), https://www.cas.go.jp/jp/seisaku/ful/bunkakai/kensa_senryaku_13.pdf
- 20 Katsuki Kurosawa, Takuya Yamagishi, Significance of counter-cluster measures, The Journal of Public Health Practice 85, 740-745, 2021
- Discussion Meeting on November 20, 2020, Discussion on lesson learned from first wave of COVID-19 pandemic in Japan – from physician’s point of view – Journal of the Japanese Society of Internal Medicine 109, 2348-2363, https://www.naika.or.jp/jsim_wp/wp-content/uploads/2020/11/nichinaishi-109-11-article_Zadankai.pdf
- Hiroshi Nishiura, Hitoshi Oshitani, Tetsuro Kobayashi, Tomoya Saito, Tomimasa Sunagawa, Tamano Matsui, Takaji Wakita, MHLW COVID-19 Response Team, Motoi Suzuki, medRxiv preprint doi: https://doi.org/10.1101/2020.02.28.20029272, April 16, 2020
- Taishi Kayano, Hiroshi Nishiura, A mathematical model for the novel coronavirus, Journal of Clinical and Experimental Medicine, 276, 20-24, 2021
- Tokyo Metropolis COVID-19 disease control and prevention measures website https://stopcovid19.metro.tokyo.lg.jp/
- Shinji Hirai, COVID-19 disease control and prevention measures – Toward the implementation of flexible infection control measures based on a point of care-oriented approach, 2nd Expert Meeting materials 3-1, 2022.5.17
- Matthew Syed, Rebel Ideas: The Power of Diverse Thinking, updated with a new chapter on the Covid-19 crisis, John Murray Press, UK, 2021
- Supervised by Ryozo Nagai & Tadatsugu Taniguchi, Aikichi Iwamoto (advisor), Recommendations for building an infectious diseases research platform towards building a country resistant to infectious diseases, Center for Research and Development Strategy, Japan Science and Technology Agency, https://www.jst.go.jp/crds/pdf/2020/RR/CRDS-FY2020-RR-05.pdf, 2020
- Dan Werb, The Invisible Siege: The Rise of Coronaviruses and the Search for a Cure, Crown, 2022
- Gregory F Albery, et. al., Climate change increases cross-species viral transmission risk, Nature, 2022 Apr 28. doi: 10.1038/s41586-022-04788-w
- Asami Hino, Account of the War Against HER-SYS – System of COVID-19 disease control and prevention measures, Takemi-Fund COVID-19 Expert Meeting, https://www.covid19-jma-medical-expert-meeting.jp/topic/7286, 2022.4.16
- Yukihiro Yamaguchi, Information sharing and operational efficiency in the COVID-19 pandemic, Takemi-Fund COVID-19 Expert Meeting, https://www.covid19-jma-medical-expert-meeting.jp/topic/7270, 2022.4.2
- Asahi Shimbun Digital, Board of Audit of Japan demands improvements in COVID-19 contact tracing app, COCOA, https://www.asahi.com/articles/ASPBW5H26PBVUTIL003.html, 2021.10.27
- The Japanese Medical Science Federation, The Committee on the Establishment of the Japan CDC (tentative name) (2nd round) (chaired by Hiroyasu Iso), Recommendations for analysis and utilization of information as well as establishment of a human resource support organization for policy recommendations aimed at health crisis management and disease control and prevention
https://www.jmsf.or.jp/uploads/media/2021/01/20210126212816.pdf, 2021.1.7 - Toru Suzuki, Reference (United Kingdom’s response), this Written Opinion
- Michiaki Masuda, COVID-19: Whence it came, to where it goes? Takemi-Fund COVID-19 Expert Meeting, 2021.12.17